Beauty & Hair Loss
Regenerative protocols targeting scalp health and hair follicle activity.
Female hair loss isn’t one single condition — it’s a symptom with many possible causes. The good news is that a lot of the common causes are treatable or manageable.
Hair loss in women is often described as “hormonal,” “genetic,” or “stress-related.” Those labels are useful, but they can hide an important point: the immune system is involved in most hair conditions, even when the hair loss is not a classic autoimmune disease like alopecia areata. One immune cell type—the macrophage—is especially important because it can help follicles restart growth, stay in a resting state, or shift toward inflammation and scarring, depending on the situation. 1

Rejuvenation Treatments
Aesthetic care at Saisei Mirai is designed to support skin and scalp health with clinic-grade protocols. Treatments are selected based on goals, skin condition, and recovery time — with a focus on natural, long-term results.
Medical-grade beauty, not “cosmetic only”
Our beauty treatments are integrated with regenerative and immune-based programs. This allows us to support not only appearance, but also tissue quality, inflammation control, and recovery processes — especially important for the scalp and hair ecosystem.
We typically combine energy-based devices, targeted injections, and scalp-focused protocols to improve firmness, tone, texture, and hair density — while keeping the outcome refined and natural.

Why the immune system matters even when hair loss isn’t “autoimmune”
Hair follicles are not isolated structures. They sit in an “immune neighborhood” (immune niche) of nearby immune cells and signaling molecules. A major review in Nature Reviews describes that hair follicles actively attract immune cells—especially macrophages and T cells—so they are close enough to influence hair follicle stem cells during normal cycling and after injury. 2
That means, seeing immune activity around a follicle does not automatically mean “autoimmune disease”. However, abnormal or chronic immune signaling can contribute to shedding, thinning, or scarring.
Macrophages are immune cells that:
- clear damaged tissue and microbes,
- coordinate repair and remodeling,
- release chemical messengers that tell nearby cells whether to “activate,” “rest,” or “repair.”
Research shows macrophages can both start and stop hair growth
Macrophages can help follicles restart growth
A PLOS Biology study showed that in mice, skin-resident macrophages decrease by apoptosis (a normal programmed process) right before hair follicle stem cells activate, and that this process is linked with Wnt signaling, a key pathway that promotes hair growth. 3
Human studies support that similar macrophage changes happen during cycling: a Journal of Investigative Dermatology paper reports that human perifollicular macrophages undergo apoptosis, express Wnt ligands, and change “polarization” during catagen (the transition phase). 4
Macrophages can also keep follicles in “rest mode”
A Cell Stem Cell study found that Oncostatin M (OSM)—a cytokine—can inhibit hair growth by signaling through JAK–STAT5 to keep hair follicle stem cells in a quiescent (resting) state. The same study identified a subset of TREM2+ dermal macrophages as a key source of OSM in resting follicles in a mouse model. 5
Immune involvement across common female hair loss types
1) Female pattern hair loss (FPHL): mostly hormonal/genetic, but often with low-grade inflammation
FPHL (gradual thinning on the top/crown, widening part) is usually driven by genetics and follicle sensitivity to hormones. However, multiple sources describe “microinflammation” and abnormal immune responses—especially around the upper follicle (infundibulum)—in androgenetic/pattern hair loss. 6
This immune activity may contribute to:
- ongoing low-level inflammatory signaling around follicles, and/or
- remodeling and fibrosis that can make follicles less able to recover.
2) Telogen effluvium (TE): immune signals often act as the trigger upstream
TE is a common cause of diffuse shedding, typically appearing 2–3 months after a trigger such as illness, fever, major stress, surgery, childbirth, or weight loss. 7
TE is not usually caused by immune cells “attacking” the follicle. Instead, systemic stress and inflammation can shift follicles into resting/shedding. Reviews discussing inflammatory states note that proinflammatory cytokines (for example IL-1 and TNF-α) can promote premature entry into catagen and increase cell stress in hair follicles. 8
3) Alopecia areata (AA): immune attack is central
AA is the best-known immune-mediated alopecia. A key concept is hair follicle “immune privilege”—a local protective state that reduces immune activation around the growing follicle. In AA, loss (“collapse”) of immune privilege is considered a major step that allows immune recognition of follicle targets. 9
T cells are often emphasized in AA, but macrophages remain part of the broader immune environment that shapes inflammation and recovery.
4) Scarring (cicatricial) alopecias: immune-driven inflammation can permanently destroy follicles
Scarring alopecias are especially important because they can lead to irreversible loss if not recognized early.
Primary cicatricial alopecias are described as inflammatory, irreversible hair loss disorders characterized by immune cell infiltrates targeting hair follicles, including lichen planopilaris (LPP), frontal fibrosing alopecia (FFA), and CCCA. 10
A classic review explains that scarring alopecia results from irreversible damage to epithelial stem cells in the bulge region of the follicle. 11
In LPP/FFA, detailed immune profiling studies specifically examine macrophage markers and macrophage polarization patterns in lesional vs nonlesional scalp. 12
FFA reviews also describe bulge immune privilege collapse and a cytotoxic T-cell–skewed inflammatory reaction against follicular regions. 13
Take-Home Points
Alopecia areata is not the only type of hair loss where the immune system is involved. Hair follicles normally depend on immune signals to cycle and repair, and macrophages are key regulators that can either support regeneration (for example via Wnt-related signaling) or maintain rest (for example via OSM/JAK–STAT signaling), and can also participate in chronic inflammation and scarring in certain conditions.
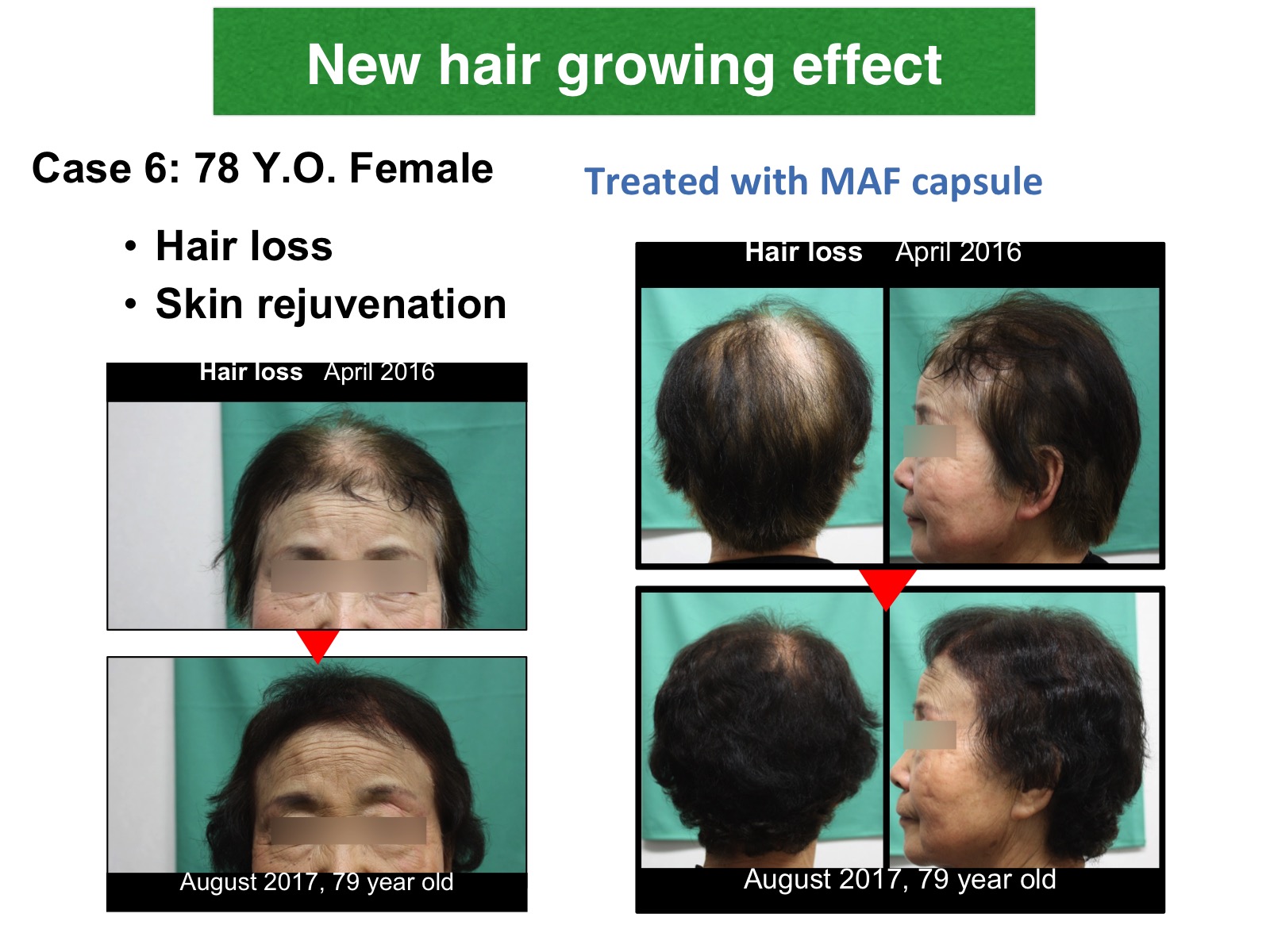
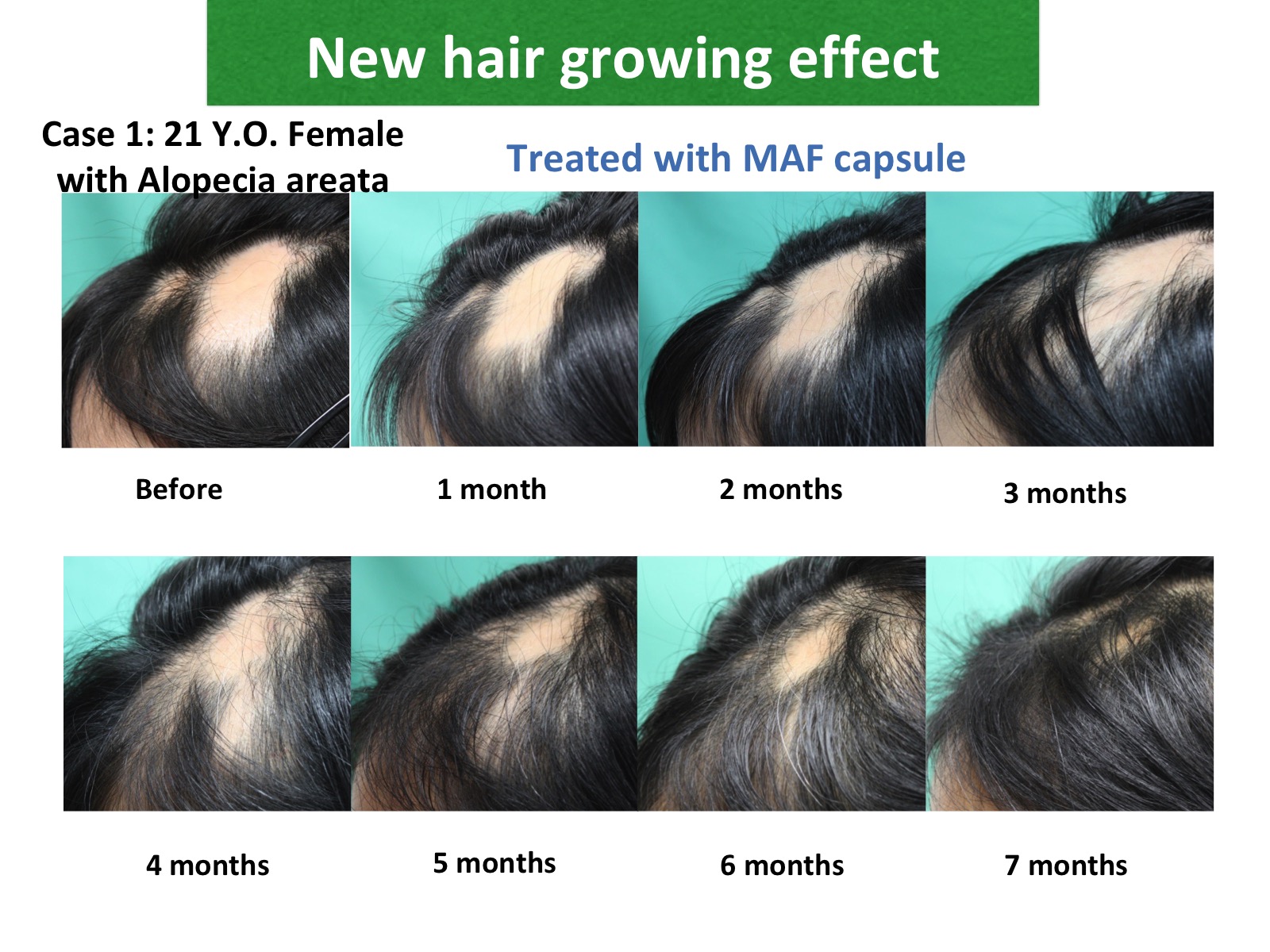
Dietary MAF: Rejuvenation Factor
Dietary MAF (Macrophage Activating Factor) is a rejuvenation factor for female hair loss.
Request an Appointment
Send a message and our team will get back to you.
Clinic
Saisei Mirai